Alcoholic Liver Disease is a syndrome of progressive inflammatory liver injury associated with long-term heavy intake of alcohol. The pathogenesis is not completely understood.
Though the alcoholic liver disease is most likely to occur in people who drink heavily over many years, the relationship between drinking and alcoholic liver disease is complex. Not all heavy drinkers develop alcoholic liver disease, and the disease can occur in people who drink only moderately.
Patients who are severely affected present with subacute onset of fever, hepatomegaly, leukocytosis, marked impairment of liver function (e.g., jaundice, coagulopathy), and manifestations of portal hypertension (e.g., ascites, hepatic encephalopathy, variceal hemorrhage). However, milder forms of alcoholic liver disease often do not cause any symptoms.
Alcoholic liver disease usually persists and progresses to cirrhosis if heavy alcohol use continues. If alcohol use ceases, the alcoholic liver disease resolves slowly over weeks to months, sometimes without permanent sequelae but often with residual cirrhosis. Of all chronic heavy drinkers, only 15–20% develop hepatitis or cirrhosis, which can occur concomitantly or in succession.
Epidemiology
Alcohol abuse is the most common cause of serious liver disease in Western societies. The true prevalence of alcoholic liver disease, especially in its milder forms, is unknown because patients may be asymptomatic and never seek medical attention.
Table of Contents
Causes
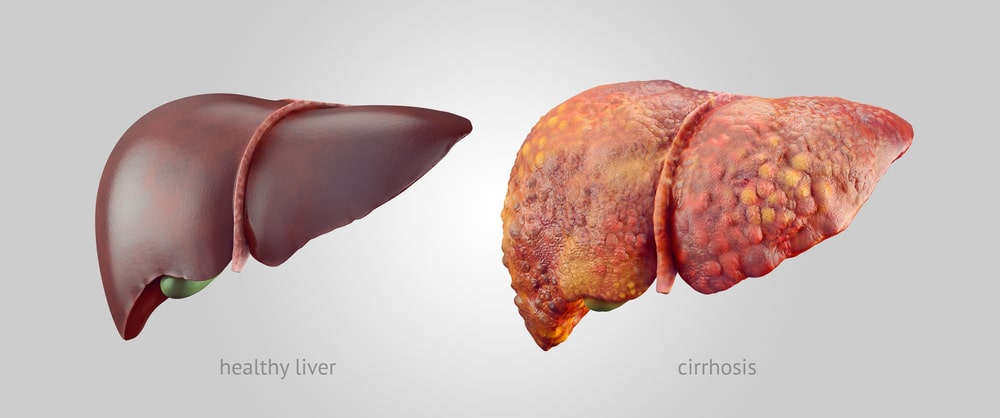
Alcoholic liver disease occurs when the liver is damaged by the excessive consumption of alcohol. How alcohol damages the liver and why it does so only in a minority of heavy drinkers is not clear. It is known that the process of breaking down ethanol; the alcohol in beer, wine, and liquor produces highly toxic chemicals, such as acetaldehyde. These chemicals trigger inflammation that destroys liver cells. Over time, web-like scars and small knots of tissue replace healthy liver tissue, interfering with the liver’s ability to function. This irreversible scarring, called cirrhosis, is the final stage of alcoholic liver disease.
Heavy alcohol use can lead to liver disease, and the risk increases with the length of time and amount of alcohol drink. But because many people who drink heavily or binge drink never develop alcoholic liver disease or cirrhosis, it is likely that factors other than alcohol play a role. These include:
Other types of hepatitis: Long-term alcohol abuse worsens the liver damage caused by other types of hepatitis, especially hepatitis C.
Malnutrition: Many people who drink heavily are malnourished, either because they eat poorly or because alcohol and its toxic by-products prevent the body from properly absorbing and breaking down nutrients, especially protein, certain vitamins, and fats. In both cases, the lack of nutrients contributes to liver cell damage.
Sex: Women have a higher risk of developing alcoholic liver disease than men do. This disparity may result from differences in the way alcohol is processed by women.
Genetic factors: A number of genetic mutations have been identified that affect the way alcohol is broken down in the body. Having one or more of these mutations may increase the risk of alcoholic liver disease.
Other factors which may increase risk include:
- Type of beverage (beer or spirits are riskier than wine)
- Binge drinking
- Obesity – Alcohol, and obesity may have a synergistic effect on the liver; that is, their combined effect is worse than the effect of either of them alone.
Pathophysiology
Some signs and pathological changes in liver histology include:
Alcoholic liver disease is characterized by the inflammation of hepatocytes. Between 10% and 35% of heavy drinkers develop alcoholic liver disease. While the development of hepatitis is not directly related to the dose of alcohol, some people seem more prone to this reaction than others. This is called alcoholic steato necrosis and the inflammation appears to predispose to liver fibrosis. Inflammatory cytokines (TNF-alpha, IL6, and IL8) are thought to be essential in the initiation and perpetuation of liver injury by inducing apoptosis and necrosis. One possible mechanism for the increased activity of TNF[1]alpha is the increased intestinal permeability due to liver disease. This facilitates the absorption of the gut-produced endotoxin into the portal circulation. The Kupffer cells of the liver then phagocytose endotoxin, stimulating the release of TNF-alpha. TNF alpha then triggers apoptotic pathways through the activation of caspases, resulting in cell death.
Mallory’s hyaline body: A condition where pre-keratin filaments accumulate in hepatocytes. This sign is not limited to alcoholic liver disease but is often characteristic.
Ballooning degeneration: Hepatocytes in the setting of alcoholic change often swell up with excess fat, water, and protein; normally these proteins are exported into the bloodstream. Accompanied by ballooning, there is necrotic damage. The swelling is capable of blocking nearby biliary ducts, leading to diffuse cholestasis.
Inflammation: Neutrophilic invasion is triggered by the necrotic changes and the presence of cellular debris within the lobules. Ordinarily, the amount of debris is removed by Kupffer cells, although in the setting of inflammation they become overloaded, allowing other white cells to spill into the parenchyma.
Chronic liver disease also shows the conditions, such as fibrosis and cirrhosis.
Fibrosis: Fibrosis of the liver is an excessive accumulation of scar tissue that results from ongoing inflammation and liver cell death that occurs in most types of chronic liver diseases. Nodules, an abnormal spherical area of cells, form as dying liver cells are replaced by regenerating cells. This regeneration of cells causes the liver to become hard. Fibrosis refers to the accumulation of tough, fibrous scar tissue in the liver.
Cirrhosis: A progressive and permanent type of fibrotic degeneration of liver tissue. Cirrhosis is a late stage of the serious liver disease marked by inflammation (swelling), fibrosis (cellular hardening), and damaged membranes preventing detoxification of chemicals in the body, ending in scarring and necrosis (cell death). Between 10% to 20% of heavy drinkers will develop cirrhosis of the liver. Acetaldehyde may be responsible for alcohol-induced fibrosis by stimulating collagen deposition by hepatic stellate cells.
Symptoms
It may not have symptoms in the early stages. Symptoms tend to be worse after a period of heavy drinking. Digestive symptoms include:
- Pain and swelling in the abdomen and tenderness,
- Decreased appetite and weight loss,
- Nausea and vomiting,
- Fatigue,
- Dry mouth and increased thirst,
- Bleeding from enlarged veins in the walls of the lower part of the esophagus.
Skin problems such as:
- Yellow color in the skin, mucus membranes, or eyes (jaundice).
- Small, red spider-like veins on the skin.
- Very dark or pale skin.
- Redness on the feet or hands.
- Itching.
Just about everyone who has the alcoholic liver disease is malnourished. Drinking large amounts of alcohol suppresses the appetite, and heavy drinkers get most of their calories in the form of alcohol.
Complications
Complications of alcoholic liver disease include:
Increased blood pressure in the portal vein: Blood from the intestine, spleen, and pancreas enters the liver through the portal vein. If scar tissue slows normal circulation through the liver, this blood backs up, leading to increased pressure within the vein (portal hypertension).
Enlarged veins (varices): When circulation through the portal vein is blocked, blood may back up into other blood vessels in the stomach and esophagus. Massive bleeding in the upper stomach or esophagus from these blood vessels is a life-threatening emergency that requires immediate medical care.
Jaundice: It occurs when the liver is not able to remove bilirubin; the residue of old red blood cells from the blood. Bilirubin builds up and is deposited in the skin and the whites of the eyes, causing a yellow color.
Hepatic encephalopathy: A liver damaged by alcoholic liver disease has trouble removing toxins from the body normally one of the liver’s key tasks. The buildup of toxins can damage the brain, leading to changes in mental state, behavior, and personality (hepatic encephalopathy). Signs and symptoms of hepatic encephalopathy include forgetfulness, confusion and mood changes, and in the most severe cases, coma.
Diagnosis
Common considerations in alcoholic patients with jaundice include chronic pancreatitis with biliary strictures and pancreaticobiliary neoplasms.
Changes in the mental status of patients with alcoholic liver disease do not always imply the presence of hepatic encephalopathy. Entities (e.g. subdural hematomas) should be excluded by obtaining a computed tomography (CT) scan of the brain.
CBC Count:
A complete blood cell (CBC) count commonly reveals some degree of neutrophilic leukocytosis with bandemia. Usually, this is moderate; however, rarely, it is severe enough to provide a leukemoid picture.
Alcohol is a direct marrow suppressant, and moderate anemia may be observed. In addition, alcohol use characteristically produces a moderate increase in mean corpuscular volume.
Thrombocytosis may be observed as part of the inflammatory response; conversely, myelosuppression or portal hypertension with splenic sequestration may produce thrombocytopenia.
Screening Blood Tests: Screening blood tests to exclude other conditions (appropriate in any patient with alcoholic liver disease) may include the following:
Hepatitis B surface antigen (HBsAg) detects hepatitis B.
Anti–hepatitis C virus by enzyme-linked immunosorbent assay (ELISA) detects hepatitis C. Ferritin and transferrin saturation detect hemochromatosis. Jaundice with fever can be caused by gallstones producing cholangitis and is suggested by a disproportionate elevation of the alkaline phosphatase (ALP) level.
Liver Function Tests: Liver enzyme levels exhibit a characteristic pattern. In most patients, the aspartate aminotransferase (AST) level is moderately elevated, whereas the alanine aminotransferase (ALT) level is in the reference range or only mildly elevated. This is the opposite of observed in most other liver diseases.
Ultrasonography: Ultrasonography is the preferred imaging study in evaluating patients with suspected alcoholic liver disease. This modality provides a good evaluation of the liver and other viscera and permits guided liver biopsy.
Liver Biopsy: Liver biopsy is not always required in the evaluation of alcoholic liver disease, but it may be useful in establishing the diagnosis, determining the presence or absence of cirrhosis, and excluding other causes of liver disease.
Treatment
In most patients with alcoholic liver disease, the illness is mild. Their short-term prognosis is good, and no specific treatment is required. Hospitalization is not always necessary. Alcohol use must be stopped, and care should be taken to ensure good nutrition; providing supplemental vitamins and minerals, including folate and thiamine, is reasonable. Patients who are coagulopathic should receive vitamin K parenterally. Anticipate symptoms of alcohol withdrawal, and manage them appropriately.
Patients with severe alcoholic liver disease may benefit over the short term from specific therapies directed toward reducing liver injury, enhancing hepatic regeneration, and suppressing inflammation. For the long term, goals include improvement of liver function, prevention of progression to cirrhosis, and reduction of mortality.
Cessation of Alcohol Intake: Cessation of alcohol use is the mainstay of treatment of alcoholic liver disease.
Liver Transplantation: Orthotopic liver transplantation is widely used in patients with end-stage liver disease. Most patients with active alcoholic liver disease are excluded from transplantation because of ongoing alcohol abuse. In most liver transplantation programs, patients must abstain from alcohol for at least 6 months before they can be considered for transplantation, and a thorough psychosocial evaluation must demonstrate that patients have a low likelihood of reverting to alcohol abuse.
Surgical Considerations:
Patients with acute alcoholic liver disease are at high risk of developing hepatic failure following general anesthesia and major surgery. Because postoperative mortality rates are high, surgery should be avoided in the setting of acute alcoholic liver disease unless it is absolutely necessary. If patients remain abstinent, the alcoholic liver disease usually resolves over time, permitting surgery to be undertaken with a substantially reduced risk.
Herbal Agents:
Milk thistle: Herbal agents have also been tried in alcoholic liver disease. Silymarin is the active ingredient in milk thistle and is a member of the flavonoids. The precise mechanism of its hepatoprotective mediation is not known, but it is probably related to its antioxidant properties. In humans with mild alcoholic liver disease, silymarin improves liver chemistry test results. Milk thistle is generally safe but can cause diarrhea and nausea.
Make sure you also check our other amazing Article on: Acute Renal Failure