
Table of Contents
What is the pharmacological action of alcohol?
Alcohol (Ethyl Alcohol/Ethanol)
The pharmacological effects of alcohol on different organs are to be considered acute and chronic.
(A) Pharmacological Effects (Acute)
Pharmacokinetics
Ethanol is rapidly absorbed from GIT. Food, especially milk delays the absorption of alcohol by slowing gastric emptying. Distribution is rapid with a Volume of distribution (Vd) of 0.5-0.7 liters/kg. It crosses BBB as well as the placental barrier, but the concentration in the brain is very close concentration to that in blood. It is because the brain receives a large proportion of blood flow.
About 95% of absorbed alcohol is metabolized and the remaining 5% is excreted through breath, urine, and sweat. Alcohol in alveolar air is in equilibrium with that in pulmonary capillary blood and this ratio is relatively constant. 80 mg/100 ml of ethanol in the blood is equivalent to 35 µg/100 ml of ethanol in expired air.
A sizable fraction of ethanol is cleared by first-pass hepatic metabolism, which follows zero-order kinetics. A fixed amount of 8-12 ml or 7-10 gm of alcohol is metabolized per hour irrespective of its blood concentration. Hence, when the stomach is empty, greater absorption produces higher pharmacological effects.
Ethanol is metabolized first to acetaldehyde and then to acetic acid. Two major pathways of alcohol metabolized to acetaldehyde, which takes place in the liver have been identified. (Fig. 1.1)
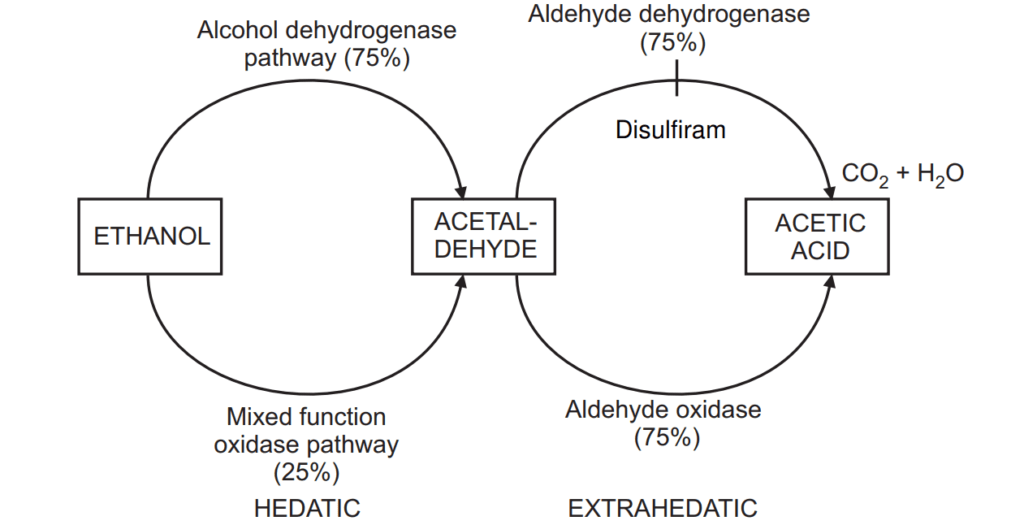
Metabolism of alcohol to acetaldehyde
The enzyme alcohol dehydrogenase, found mainly in the liver, stomach, and intestine oxidizes about 75% ethanol to acetaldehyde (Fig. 4.10). The metabolism follows zero-order kinetics.
Another enzyme, the mixed function oxidase (CYP450) system is responsible for the remaining 25% of ethanol metabolism. At a concentration of ethanol above 100 mg/dl, this pathway is more important for metabolism. During chronic alcohol use, there is induction of this enzyme system and therefore metabolism of steroids, oral anticoagulants, and paracetamol is increased.
Metabolism of acetaldehyde to acetic acid
About 75-80% of acetaldehyde is converted to acetate in the liver by the enzyme aldehyde dehydrogenase (ALDH). Only 20-25% of acetaldehyde is converted to acetic acid outside the liver by an enzyme aldehyde oxidase. This leads to the formation of acetate which is further metabolized to CO2 and water.
On CNS
Alcohol enhances the action of GABA at GABAA receptors similar to that of benzodiazepines (BZDs). BZDs also intensify the acute effects of alcohol. BZD antagonist, Flumazenil reverses the CNS depressant action of alcohol; however, it is not used to reverse ethanol intoxication. Ethanol also inhibits the ability of glutamate to activate the NMDA receptor and thus inhibits the opening of the calcium channel linked to the NMDA receptor. The acute effects of alcohol on CNS are sedation, relief from anxiety, loss of inhibitions, and impaired judgment as well as driving skills. These effects occur at alcohol blood levels between 50-100 mg/dl. Blood levels of 120-160 mg/dl lead to effects like ataxia, slurred speech, mental clouding, and grossly impaired motor functions. These effects are identified as “gross drunkenness”. Levels between 200-300 mg/dl produce emesis and stupor, while levels above 300 mg/dl lead to coma and respiratory and cardiovascular depression. Levels above 500 mg/dl are lethal. Concomitant administration of drugs like BZDs, Phenothiazines, Tricyclic antidepressants, and opiates causes additive depression.
On Heart
At blood concentrations of 100 mg/dl, ethanol decreases myocardial contractility. Acetaldehyde may cause cardiac abnormalities by altering myocardial stores of catecholamines. Large doses depress the vasomotor center leading to a fall in BP.
Smooth muscles and other effects
- Ethanol causes cutaneous vasodilatation, which leads to a feeling of warmth, but actually increases heat loss.
- It produces relaxation of the uterus only at high doses.
- Diuresis is associated with alcohol intake. It is caused by the inhibition of antidiuretic hormone secretion and partly because of increased water intake. However, tolerance develops rapidly to diuresis.
- Aggressive sexual behavior is due to loss of inhibitions; however, the performance of the sexual act is hampered.
- Moderate amounts of ethanol cause catecholamine release and reduce glucose uptake by the tissues resulting in hyperglycemia. However, inhibition of gluconeogenesis can also cause hypoglycemia.
- It requires no digestion and instantly supplies 7 cal/gm. This energy cannot be stored or utilized for bodybuilding. Thus, alcohol serves as an expensive as well as nutritionally worthless food.
(B) Pharmacological Effects (Chronic)
Chronic ethanol intake adversely affects the functions of several vital organs.
Nervous system
Tolerance and dependence are major effects on CNS. Tolerance develops to the subjective and behavioral effects of alcohol. Chronic alcoholics may function normally even above 180 mg/dl levels as compared to occasional drinkers. The reduced rate of absorption and faster metabolism are responsible for pharmacokinetic tolerance.
Chronic alcohol drinkers, if forced to abstain, experience distressing withdrawal symptoms with physical dependence. The symptoms include hyper-excitability, toxic psychosis, delirium tremens, and seizures. The withdrawal effects are observed around 8-24 hours after abstinence. The symptoms are tremors, nausea, and sweating. This phase is followed by seizures and in the next three days delirium tremens develops, which is characterized by confusion, agitation, aggressiveness, and hallucination. Psychological dependence is characterized by a compulsive desire to drink.
Neurotoxicity
Chronic/heavy drinkers show ataxia, dementia, and peripheral neuropathies. It is associated with thiamine (vitamin B1) deficiency. The syndrome is characterized by ataxia, confusion, and paralysis of extraocular muscles. Prompt treatment with IV/IM thiamine is necessary. Alcohol also impairs visual acuity with a painless blurring of vision on chronic consumption.
Liver and GIT
Chronic excessive ethanol consumption causes fatty liver with inflammation. It leads to irreversible hepatic necrosis, fibrosis, and failure. Another factor causing liver damage is malnutrition. Women appear to be more susceptible to alcohol hepatotoxicity. It is one of the most common causes of chronic pancreatitis. Irritation, inflammation, bleeding, scarring, or even induration of gut mucosa occurs after chronic alcohol use. Defective absorption leads to a deficiency of water-soluble vitamins.
Cardiovascular system
Chronic alcohol consumption leads to dilated cardiomyopathy, ventricular hypertrophy, and fibrosis. Alcohol also interferes with the therapeutic benefits of β-blockers and ACE inhibitors. It is also associated with ventricular arrhythmia, which may lead to syncope. It is also a contributory factor for hypertension.
Blood lipoprotein and platelet function
Moderate alcohol intake increases HDL and decreases LDL, which may account for the observed protective effect against ischaemic heart disease. Alcohol inhibits platelet aggregation; it results from the inhibition of arachidonic acid formation from phospholipids. Chronic alcoholics show megaloblastic anemia due to alcohol-related folic acid deficiency. Iron deficiency anemia may be caused by gastrointestinal bleeding.
Endocrine effects and electrolyte balance
Chronic alcoholism can produce testicular atrophy, gynecomastia, and impotence. “Pseudo-Cushing’s syndrome” is observed in chronic alcoholics. Alcoholics with cirrhotic liver may show ascites, edema, and effusions due to decreased protein synthesis and portal hypertension. Secondary aldosteronism in chronic alcoholics can cause hypokalemia and muscle weakness. Some alcoholics may exhibit ketosis caused by increased lipolytic factors like cortisol and growth hormone.
Effects on fetal development
Consumption of about 6-10 units of alcohol per day during pregnancy causes fetal alcohol syndrome. It is characterized by microcephaly, mental retardation, flattened face, retarded growth, and cardiac or other malformations of eyes and ears as congenital abnormalities.
Another lesser degree of impairment is “alcohol-related neuro-developmental disorder”. It is characterized by behavioral as well as cognitive and motor defects.
Miscellaneous effects
- There are effects on the immune system. Chronic alcoholics are pre-disposed to lung infections and may suffer from pneumonia.
- Its chronic use is associated with an increased incidence of neoplastic diseases like breast and liver carcinoma.
- Ethanol alters uric acid metabolism by increasing uric acid metabolism and decreasing renal secretion. Hence, gout may be precipitated due to hyperuricemia.
Treatment of Acute and Chronic Alcoholism
Intoxication due to acute intake of ethanol is managed by the maintenance of vital signs and prevention of aspiration of vomitus. Treatment of hypoglycemia and ketosis can be made by giving IV glucose. IV/IM thiamine and correction of electrolytes may also be required.
The abstinence syndrome is managed by the administration of a long-acting sedative – hypnotic like Chlordiazepoxide or Diazepam. The intensity of withdrawal syndrome may be reduced by Clonidine and Propranolol. Once the withdrawal phase is over, BZDs may be withdrawn with a gradual reduction of the dose. Several months may be needed for the restoration of normal sleep, and the decrease of tremors and anxiety.
Alcohol dependence is followed by the following means:
- The first effort is to render ethanol consumption unpleasant. It is discussed under the use of Disulfiram.
- Another approach is to reduce craving or to blunt the pleasurable outcome of renewed drinking. Naltrexone, an opioid antagonist in a dose of 50 mg once a day is used to treat alcohol dependence. It reduces the craving for alcohol. Another approach is to use an anticonvulsant drug like Topiramate. The drug potentiates the inhibitory effects of GABA but acts at a site different from BZDs or barbiturates.
- Selective serotonin uptake inhibitors (SSRIs) like Fluoxetine can increase serotonergic activity in CNS. Alternatively, Ondansetron, a 5-HT3 antagonist has been successfully used to treat alcohol dependence.
- To reduce the craving for alcohol Acamprosate has been tried. It reduces the excitatory effect of glutamate on the NMDA receptor and also facilitates GABA neurotransmission. It also possesses some opioid antagonist activity and increases serotonin levels in synapses.

Drug Interactions
- Chronic consumption of alcohol increases the risk of hepatotoxicity by Paracetamol. It involves CYP2E1 mediated conversion of paracetamol to reactive hepatotoxic metabolite N-acetyl-p-benzo-quinone imine.
- All cerebral depressants like hypnotics, sedatives, phenothiazines, and antihistamines can have a synergistic effect with ethanol. It can have serious consequences during driving.
- Chronic alcoholics are relatively tolerant to the use of general anesthetics like halothane.
- Alcohol enhances the hypoglycaemic effects of insulin and sulfonylureas.
- Some alcoholic drinks like beer or wine contain tyramine, which is sufficient to cause hypertensive crisis in patients taking MAO inhibitors.
Clinical Uses of Ethanol
It is used for the following purposes:
- As a skin antiseptic (76% v/v), alcohol is the most effective.
- It has an astringent action and hardens the skin to prevent bed sores.
- It is used to treat methanol poisoning.
Disulfiram
What is the action of disulfiram in pharmacology?
The enzyme aldehyde dehydrogenase is inhibited by Disulfiram and by other drugs including metronidazole, oral hypoglycemics, some cephalosporins like Cifotetan and Cefoperazone and urinary antiseptics like Nitrofurantoin. When alcohol is consumed in presence of Disulfiram, the conversion of acetaldehyde to acetic acid is significantly reduced.
Hence, acetaldehyde accumulates to cause effects like facial flushing, nausea, vomiting, dizziness, and headache. The reaction is extremely unpleasant, but not life-threatening. Hence, Disulfiram can be used as an aversion therapy to discourage people from consuming alcohol. Disulfiram is rarely used as an aversion therapy for alcohol dependence. Adverse reactions of Disulfiram include skin rashes, metallic taste, and abdominal upset. Its dose is 1 gm on the first day which is to be reduced by 250 mg daily until 250 mg once the daily maintenance dose is adjusted.
Disulfiram: ANTADICT, SUFITAL, ESPERAL is available as 250 mg tablet.
Make sure you also check our other amazing Article on: How do you evaluate analgesic activity in mice?